

The American Diabetes Association (ADA) published another update to its standards. What’s the ADA Diabetes Standards of Care and why is it important?
For over 30 years, this living document has been developed by the ADA. It is important because it looks at research conducted over the last year to learn and share what the best quality of care is for people with diabetes. To assure impartiality, more than half of the professionals that review the research have no industry-related conflicts of interest.
So, every year (or more often, if significant new evidence comes to light), the Professional Practice Committee of the ADA updates its Standards of Care document. The ADA reviews the research from the past year and makes recommendations for changes in patient care based on the new findings. The recommendations go through an internal review and an expert evaluation, after which they have to be approved by their Board of Directors. The whole process is funded by the ADA, without sponsorship.
Individual Risk, Individualized Care
This year’s Diabetes Standards of Care feature some interesting changes. In a webinar presenting the 2022 standards, Robert Gabbay (MD PhD), Chief Scientist and Medical Officer of the ADA, said a common thread among many of the updated guidelines could be summarized as, “One size does not fit all.” Many of the guidelines emphasize looking at the person in the context of their lives and of their individual risk factors. Here are some of the highlights.
New Standards for Diagnosis
Undiagnosed diabetes is a significant problem. This year, the ADA lowered the age to begin screening for Type 2 diabetes from 45 to 35, based on evidence that diabetes is appearing in younger people. In fact, they recommend testing anyone over the age of 18 with known risk factors (including ethnicity and lifestyle), and all women who are planning to become pregnant or who are pregnant. People who test normal should be re-screened every three years or more often if they become symptomatic.
They also recommend counseling first degree relatives of people with Type 1 diabetes about the disease and on their increased risk. Anyone diagnosed under the age of 6 months should be genetically tested.
Prevention: Include Comorbidities in the Picture
The ADA wants physicians to be involved in preventing or delaying the onset of Type 2 in vulnerable people by paying particular attention to each person’s risk. They suggest beginning diabetes prevention measures for anyone at elevated risk for developing diabetes because diabetes impacts is linked to comorbid conditions like cardiovascular and kidney diseases. (By the way, they recommend that all patients get their COVID-19 vaccine.)
Support Wellbeing: Healthy Carbs, Tech Tools
Dr. Gabbay highlighted two points in a chapter on Facilitating Behavior Change. One recommends teaching clients about the quality of carbs, not just their numbers. It’s important to encourage choosing quality carbohydrates, such as whole grains and less processed foods.
The guidelines also support technologies for diabetes control, including mobile apps and digital coaching. To further individualize care, research indicates that cognitive evaluations might help some patients and their caregivers determine which technologies are most appropriate for them.
Hitting the Glycemic Targets Through Using Technology
For those using a continuous glucose monitor (CGM), the recommendations also include regular blood glucose monitoring (BGM), both for calibrating the CGM and in case the CGM fails.
Using technology like CGM is important for patients to track their Time in Range and Time Out of Range, factors that are useful in treatment adjustments. However, individual ability comes into play again here: These tools should only be used if the person knows how to use them safely. Even youths with T1 who take multiple injections or continuous subcutaneous insulin can benefit from CGM and other technologies if they can use them safely.
For dosing, insulin pens are preferred, but syringes are also fine if the patient or caregiver prefers them. Doctors have to be aware that patient preferences affect the person’s success at self-care.
Treatment Depends on the Person
For treatment of both Type 1 and Type 2 diabetes, the guidelines emphasize that every aspect needs to be taken into consideration: patient-caregiver preference, insulin type and dosing regimen, the cost, that person’s risk of comorbidities, and the person’s capability. For example, with Type 2, metformin is still the first-line medication – it should even be considered for people who are prediabetic – but there are some people for whom it is not the best treatment given their comorbidities. The evidence says that not everyone needs metformin.
Combination Medications from the Start: GLP-1 and SGLT2
Chapter 9 of the standards says that starting therapy with a combination of medications is appropriate:
- Other medications (glucagon-like peptide 1 [GLP-1] receptor agonists, sodium–glucose cotransporter 2 [SGLT2] inhibitors), with or without metformin… are appropriate initial therapy for individuals with type 2 diabetes with or at high risk for atherosclerotic cardiovascular disease (ASCVD), HF (heart failure), and/or chronic kidney disease (CKD).
They also say that for patients with Type 2, a GLP-1 receptor agonist is preferred to insulin when possible. If insulin is used, it should be used with a GLP-1 receptor agonist “for greater efficacy and durability of treatment effect.”
Statins
Statins are also appropriate for some cases. The updated guidelines say patients with diabetes aged 40–75 years without ASCVD (Atherosclerotic Cardiovascular Disease) should be taking moderate-intensity statins alongside their lifestyle therapy.
Managing All the Risks
Diabetes care is more than just managing blood sugar. Chapter 10 of the Standards of Care again emphasizes that diabetic complications are part of treating the whole person. It uses this graphic to illustrate the concept of four pillars of care:
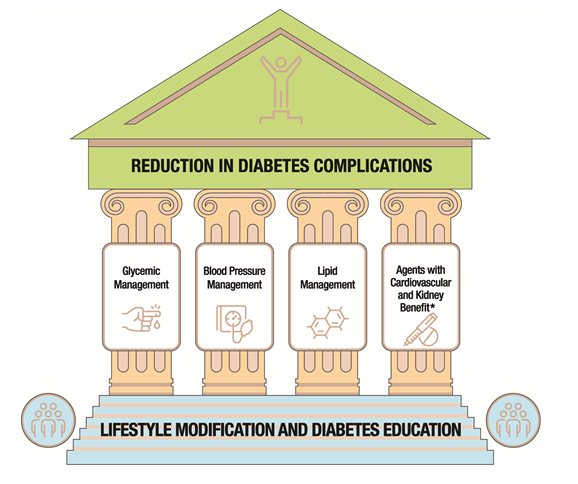
Diabetes care relies on a foundation of lifestyle modification and diabetes education, but supporting the whole individual relies on four factors to reduce complications: Managing sugars, blood pressure, and fats along with taking preventative medications for cardiovascular and kidney diseases.
The Person is More than the Disease
The Diabetes Standards of Care repeatedly emphasize that physicians consider each patient’s preferences, individual risk, and lifestyle: Can this person use this technology? What changes do they need to make if they’re pregnant, in a hospital, have medical issues that affect their ability to swallow? What is this person’s insurance coverage, can they afford the treatment you want to recommend? For 2022, the ADA recommends that a person’s health care team look beyond the A1c number, and see each person in their long-term journey managing diabetes.
Sources:
Standards of Care 2022 Webinar
Abridged Diabetes Standards of Care
Standards of Medical Care in Diabetes – 2022
Image by Mohamed Hassan from Pixabay



