

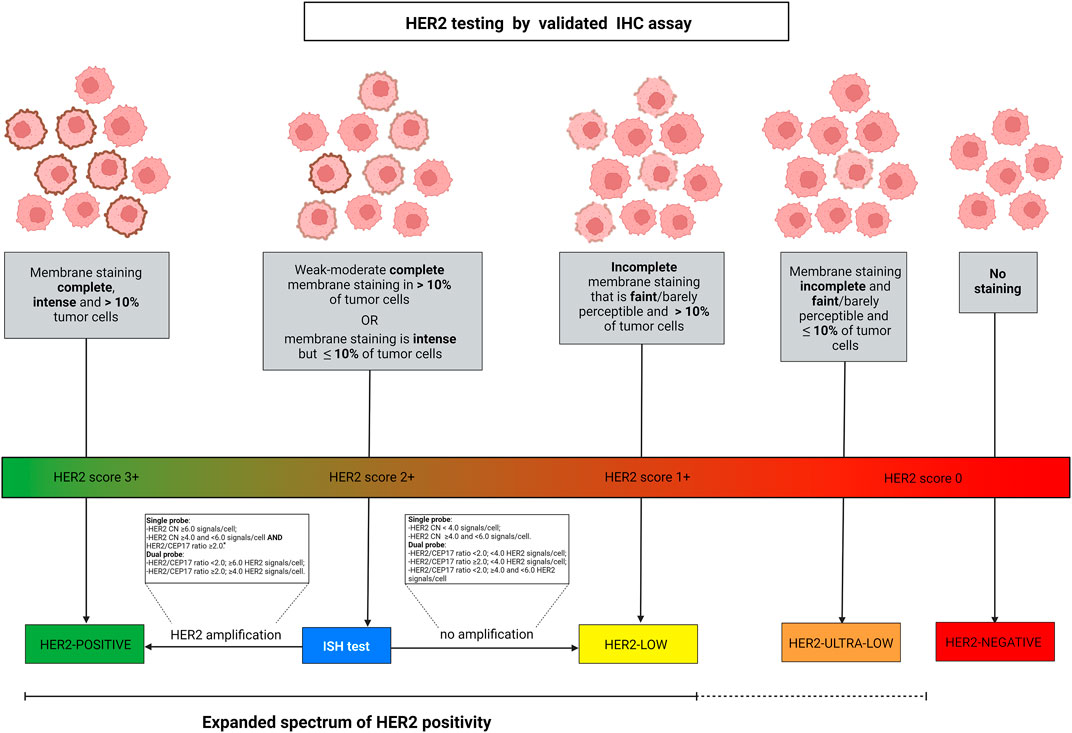
Each year in the United States, approximately 264,000 women and 2,400 men are diagnosed with breast cancer. Of those people, about 30% will go on to develop metastatic breast cancer (cancer that has spread beyond the breast, often to the brain, lungs, bones, or liver). Biopsies of breast cancer tissue determine if the surface of the cancer cells contain an elevated amount of a protein, called HER2, which is involved in controlling cell reproduction. Until now, breast cancers were generally divided into just two categories for treatment: HER-positive or HER-negative. [1][2][3]
HER2-positive or HER2-negative
Targeted treatments are available for HER2-positive tumors, but these drugs didn’t have much of an effect on people categorized as HER2-negative. While HER2-positive cancers are considered more aggressive, many of the targeted drugs flag the presence of HER2 proteins on the surface of cells so that the immune system is better able to choose them for destruction. When HER2 isn’t present, or isn’t present in large amounts, the “HER2-negative” people weren’t treated with the targeted therapies. The rationale was that there weren’t enough “flags” on the tumor cells for those drugs to be effective. [4]
Now: HER-low
However, many of those people’s cancers still express some HER2. Now, a presentation made at the ASCO conference in June is likely to fine-tune standard treatment categories from HER positive or negative to include “HER2-low.” New research indicates that it is now possible to detect lower levels of HER2 in patients. The research team also showed that a specific category of drug both targets the protein and delivers a payload that destroys not just that cell, but the cancer cells around it. These results are likely to change the way in which women and men are tested and treated. [4][5][6]
New Treatment Significantly Outperforms Chemo
Dr. Shanu Modi, medical oncologist in the Breast Medicine Service at Memorial Sloan Kettering, presented the results of the DESTINY-Breast04 phase 3 clinical trial. The trial participants had HER2-low metastatic breast cancer and had all been treated with at least 1 round of chemotherapy. The trial compared treating participants with an antibody drug conjugate (ADC) called trastuzumab deruxtecan (T-DXd) against a group receiving their physician’s choice of treatment, typically single-agent chemotherapy.
The results show that the antibody-drug conjugate (ADC), T-DXd, prolonged both progression-free survival (PFS) and overall survival (OS) better than chemotherapy.
Based on the year and a half follow-up, T-DXd gave patients a 50% reduction in the risk of disease progression or death (PFS: 9.9 vs 5.1 months), and a 36% reduction in the risk of death (median OS: 23.4 vs 16.8 months). [5]
What is an antibody drug conjugate (ADC)?
An antibody is a molecule that attaches to a protein on the surface of a cell called an antigen. HER2 is an example of an antigen. Antibodies are specific to each antigen. Trastuzumab is a lab-manufactured antibody (monoclonal antibody) that attaches to HER2 cancer cells. However, it is a type of monoclonal antibody that also carries a drug with it, called an “antibody drug conjugate.” An antibody drug conjugate not only attaches to the cell, it delivers a drug directly to that cell. (Here’s an excellent short video on how they work.)
T-DXd Flags and Delivers
Trastuzumab is the monoclonal antibody typically used to treat HER2-positive cancers by flagging those particular cells, but the ADC goes one step further by delivering the powerful chemotherapy drug, deruxtecan, right to the cell, causing catastrophic DNA damage. [5]
With a mechanism called “bystander effect,” the deruxtecan also kills neighboring tumor cells. “This bystander antitumor effect, offered by the optimized ADC technology, potentially drives T-DXd activity in patients with varying and low levels of HER2,” Dr. Modi said.[5][7]
Who does this help?
We know that using T-DXd is more effective even on low levels of HER2 expression due to drug and bystander effect, but just how many people fall into this category? More than 60% of HER2-negative metastatic breast cancer patients, according to Dr. Modi. “Approximately 60% of HER2-negative metastatic breast cancers express low levels of HER2, yet these have always been defined and treated as HER2-negative breast cancers, where treatment choice is guided by the hormone receptor status,” she said.
“Traditionally, we would have offered patients in this setting single-agent palliative chemotherapy. However, we can now offer these patients the opportunity to receive a targeted therapy that is associated with superior outcomes and a survival advantage.” [8]
Increased sensitivity of testing for presence of low levels of HER2, formerly considered untargetable, supports treating a much broader group of women with breast cancer. The DESTINY-Breast04 results also show the remarkable potential effectiveness for other ADCs, and shows that improvements in sensitivity testing of all kinds will reveal more targets for healing.
References
[1]https://www.cdc.gov/cancer/breast/basic_info/index.htm
[2]https://www.breastcancer.org/types/metastatic
[3]https://www.cancer.gov/publications/dictionaries/cancer-terms/def/her2
[4]https://www.frontiersin.org/articles/10.3389/fmolb.2022.834651/full#B62
[7]https://dailynews.ascopubs.org/do/10.1200/ADN.22.201047/full/
[8]https://www.onclive.com/view/trastuzumab-deruxtecan-is-new-standard-of-care-for-her2-low-mbc
Image by skylarvision from Pixabay





{kind=link}